


Cholestasis and Listening to Your Intuition: Podcast Episode #261

Jenn Johnson shares her personal pregnancy stories and discusses how even as a nurse she had to advocate for herself during pregnancy. Jenn also shared info on her book, A Nurse’s Happy Place. Hello, hello! This is Kristin with Ask the Doulas, and I am thrilled to chat with Jenn Johnson today. Jenn is the owner […]
How to Build Your Birth and Postpartum Support Team

Kristin Revere was a guest on the Plus Mommy podcast to talk about setting yourself up for success by creating a strong support team for birth and postpartum. Listen to the podcast here. A strong support team can significantly impact your overall experience and well-being, from physical and emotional support to guidance through the complexities […]
How to Prepare for Birth and Postpartum with Kristin Revere
Kristin Revere spoke about the new book Supported as a guest on the kozekoze podcast with Garrett Kusmierz. Here’s their conversation. Listen to the podcast! Welcome back to the kozekoze podcast, and happy Mother’s Day! Wow, what a day. This is my fourth Mother’s Day, which sounds really crazy. I cannot believe I have a […]
The Importance of Support in the Pre and Postpartum Period with Kristin Revere
Kristin Revere and Meaghan Beames chat about support in the pre and postpartum period Meaghan is the host of The MyBaby Craniosacral Podcast. “It’s all about knowing options and building your own dream team of professionals based on however you choose to birth your baby and parent your baby.” Kristin Revere, owner of Gold Coast Doulas, […]
Breastfeeding and Pumping Tips from Daniela of SOLMA Tea: Podcast Episode #225

Kristin Revere and Daniela Procopio discuss how her breastfeeding journey led her to create SOLMA Tea. She also shares tips for support and balance as both a mother and an entrepreneur. Hello, hello! This is Kristin Revere with Ask the Doulas, and I am here to chat with Daniela Procopio. Daniela is the founder […]
Your Options for Birth and Postpartum Doula support with Kristin Revere: Podcast Episode #206

Kristin Revere of Gold Coast Doulas talks about the types of birth and postpartum doula business models. She also talks about the role of a newborn care specialist. Ask The Doulas Podcast · Your Options for Birth and Postpartum Doula support with Kristin Revere Hello! This is Kristin Revere with Ask the Doulas, and today […]
8th annual Diaper Drive
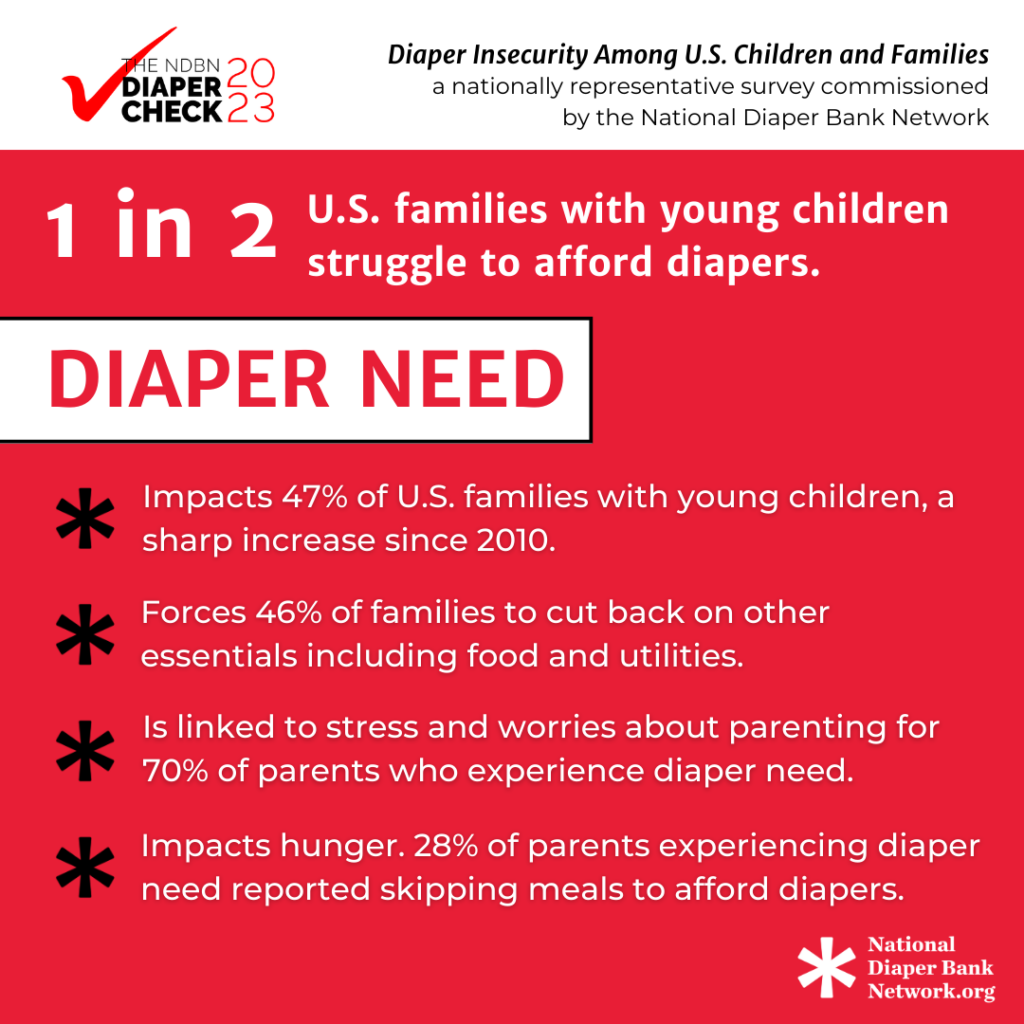
Gold Coast Doulas is holding our 8th annual Diaper Drive from September 1st to October 1st, 2023. Giving back is an important foundation of our business as a Certified B Corporation; clean diapers make a significant impact on the health of new families and our giving focus is on supporting low-income women and children. One in […]
Medicaid for Doulas with Doulas Diversified: Podcast Episode #168

Kristin chats with Erica about the Medicaid coverage for doulas in Michigan and how this improves maternal and infant health outcomes. You can listen to this complete podcast episode on iTunes, SoundCloud, or wherever you find your podcasts. Ask The Doulas Podcast · Medicaid for Doulas with Erica Guthaus of Doulas Diversified Welcome. You’re […]